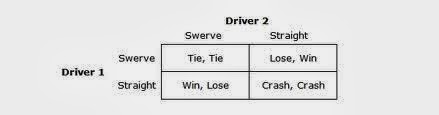
Do you recall the old game of chicken? Two cars (driven by slightly crazy people) drive towards each other at high speed. The person who swerves first--to avoid the pending collision--is "chicken" and loses.
If we look at this as a problem in decision analysis, we find the following matrix of possible results.
The question often posed about this game is how you can guarantee that you will win, but also guarantee that you don't end up "winning" by crashing into the other person, who has also "won."
The solution is quite simple. As you approach the other car, you pull the steering wheel off its column and--making sure the other person sees you do it--you throw it out of the window. The other driver now knows that there is no way for you to veer off, and there is a very high likelihood that s/he will be "the chicken" and turn away.
Many cities and towns and states across the country face a big problem called "Other Post-Employment Benefits." These benefits are a promise made to public employees that their government entity will pay for their health care insurance after retirement, supplementing Medicare until the day they or their spouse dies. OPEB represents a huge future liability for local governments, with amounts well in excess of their willingness to pay to build up an appropriate level of reserves. In my city, for example, the unfunded OPEB amount is about
$600 million (equal to two years of the entire city budget.) About 90,000 people live here, and that amount of money represents an extra mortgage of about $18,000 for each of the 33,000 households in the town. (According to
this article, the statewide unfunded obligation for Massachusetts cities and towns is $26 billion, a mortgage, again of $4000 for every man, woman, and child living in the state.)
The pattern across America is to ignore this problem or apply band-aids. At best, local administrations put in place a savings fund for new employees or reduce future benefits for this cohort, so they don't add as much to the problem going forward. But there are actually very few new employees. Meanwhile, the localities have to engage in a pay-as-you-go policy for current retirees. But they don't plan very well for the fact that even the current retirees are likely to need more and more expensive care over time, draining the municipality as it tries to keep up with the pay-as-you-go plan. More importantly, most have no plan whatsoever to deal with the large number of incumbent employees who will be added to the OPEB rolls as they retire.
Relatively new
accounting standards from the Governmental Accounting Standards Board (GASB) Statement No. 45 provide for the recording of OPEB expense and the liabilities in the financial reports of state and local government employers. But those standards
do not require governments to solve the problem.
So, the way most localities are dealing with this problem is by playing chicken and throwing out the steering wheel. They don't like to say this publicly, but they fully expect that, when the time comes, the federal government will rescue them from this situation. Indeed, the more localities that choose to play chicken, the more likely this will be the result. The last thing the US government would want is to have dozens or hundreds or thousands of local government entities going into default. The political pressure from retirees, local taxpayers, and local governments will come down on Congress to solve the problem. (This possibility is acknowledged in a
2011 Congressional Budget Office study.)
What makes this all so risky and difficult is that it will be occurring precisely when the funding for Medicare--for non-government retirees--also gets very tight because of the country's demographic trends.
A better plan would be to have the federal government impose the kind of standards it does on private companies, requiring localities to fully fund OPEB liabilities. Give the local governments a period of time to catch up, but don't let them engage in this kind of game of chicken.